We use cookies to improve your experience.
Learn more.
by Tricia Arculus
PTNS uses acupuncture and electro-stimulation to stimulate the posterior tibial nerve, which innervates the sacral plexus at the base of the spine which in turn controls bladder and pelvic floor and is responsible for its function.
The electric current is a continuous square waved form with a duration of 200 micro seconds and a frequency of 20 Hertz. The tibial nerve runs down the inside of the leg, along the spleen and kidney channels, and into the foot. Hence stimulation of this nerve causes a retrograde stimulation of the sacral nerve plexus (neuromodulation).
PTNS is believed to correct misinformation travelling between the brain and the organs supplied by the nerves from the sacral plexus (S2-S5) thus affecting function of the nerves supplying the bladder, external anal sphincter, genitalia and pelvic floor muscles.

Typically PTNS therapy involves 12 consecutive 20- 30 minute treatments given 1-3 times a week. Research shows no difference in the final outcome if done 3 times or once a week, it will just shorten or lengthen the time in which symptoms are reduced. 2 fine-gauge needles are inserted percutaneously just above the medial ankle, next to the tibial nerve and the other just on the inner aspect of the arch of the same foot.
The needles are connected to a low-voltage stimulator. Stimulation of the posterior tibial nerve produces a typical motor (plantar flexion or fanning of the toes) and sensory (tingling in the ankle, foot or toes) response.
Intensity is determined by the highest level tolerated by the patient, who holds the stimulator to adjust the intensity. Occasionally patients return for top up treatments which are believed to increase longevity of the results.

No different to those associated with acupuncture or electro-acupuncture These are reported as mild or transient and uncommon, effecting 1-2% and include minor bruising, bleeding, tingling and mild pain at the needle site. These side effects seem minor in comparison to side effects from medication used to treat OAB which range from 9.7 – 63 percent including constipation, dry mouth, impaired urination and urinary tract infections. This high rate of side effects from traditional medications is thought to be a likely a reason why patients often stop their medication (10). In a study of 220 patients who had PTNS, there were 5 instances of side-effects(25).
There are no major safety concerns in treating OAB, FI, CPP or PBS.
Contra-indications are the same as for those for electro-acupuncture, and not used on patients with a history of epilepsy or seizures, severe heart disease, strokes, pregnancy or on patients with pacemakers. If a patient has a difficult time tolerating needling then adjustments should be made and then consideration of discontinuance of treatment if no alleviation of discomfort during treatment can be found.
Precautions that need consideration include metal allergies, fragile or infected skin at site for needle insertion, anticoagulant use or blood disorders, mental health history, trying to conceive, unstable blood pressure, unstable diabetes and a history of cancer.
Indications for use of PTNS:
Its popularity is set to increase with the advent of implantable PTNS devices, although these are still in research phase.
Defined as urinary urgency, with or without urge incontinence, usually with frequency and nocturia. OAB is a condition affecting adults and children worldwide. Its cause, often unknown, but may be due to numerous factors or traumas such as childbirth, prolapse, prostate enlargement, poor pelvic floor muscle control and more. It may sometimes be associated with other conditions that may cause similar symptoms and need to be ruled out, e.g.
In a normally functioning bladder the detrusor muscle in the bladder wall remains relaxed during the final filling phase and only contracts when about to void and the bladder is over half full. In OAB the detrusor muscle starts to contract inappropriately early which causes the sudden and strong desire to void and can lead to leakage or incontinence. It can cause a significant psychological burden, be incredibly bothersome and have a huge negative impact on quality of life.
A total of 53 studies encompassing 610,438 participants in an analysis determined the global prevalence of OAB to be 20 % (3). This study also showed the prevalence of OAB to have increased over the last 20 yrs and to be higher in obese individuals, women and those over 60 yrs old. It also has higher prevalence rates among middle-income countries compared to higher-income countries.
Include bladder training, pelvic floor muscle training, Frequency Specific micro current (FSM), anticholinergic drugs, Botulinum toxin injection, sacral nerve stimulation or less commonly surgical options including bladder reconstruction and urinary diversion.
Defined as the involuntary passage of flatus (wind) or faeces (stool). The underlying cause is often complex with multiple potential contributing factors including anorectal structural abnormalities, neurological disorders, cognitive or behavioural dysfunction, stool consistency, or general disability (particularly age) and sometimes no cause can be found. Patients often find it difficult to seek help, partly because of anxiety about the possible underlying cause and because symptoms can be so distressing that they are embarrassed to talk about them. Having faecal incontinence can have substantial social, psychological and employment related consequences for patients, and can affect their relationships with others, including partners and children, thus having a significant effect on quality of life, confidence and psychological wellbeing
The exact prevalence is difficult to establish due to the fact that it is a stigmatizing condition that may be under reported and also due to differences in the definition. It is however extremely common, estimated to affect up to 10% of adults, while rates in people residing in care homes are estimated at up to 60% and liquid stool is up to 3 times more common than solid (4). Also found to be more prevalent and more severe in older people but there are no significant difference in prevalence between men and women.
include education, life style alterations (reduction of smoking, low caffeine, weight loss), protection, skin care, pelvic floor muscle training, bowel retraining, specialist dietary assessment and management, biofeedback, stool building agents, anti-diarrhoeal medications (loperamide).
2nd line non-surgical management: PTNS, Frequency Specific Microcurrent (FSM), trans anal irrigation, anal inserts.
2nd line Surgical management: Sarcral nerve modulation, bulking agents, sphincteroplasty, neosphincter (stoma) formation (21).
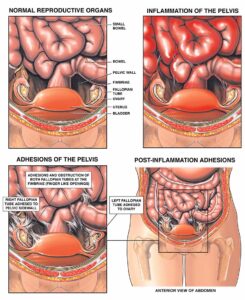
CPP, which occurs in both men in women, is defined as constant or episodic abdominal or pelvic pain, hypersensitivity or discomfort lasting longer than 6 months, usually associated with elimination changes and sexual discomfort in the absence of organic causes (32). Symptoms can actually be anywhere between the umbilicus and the thighs.
Chronic pelvic pain syndrome (CPPS), a sub-division of CPP, is generally defined as pain in the pelvic area that persisted for 3–6 months or longer. The pain can be functionally disabling, often leading to central sensitization, which enhances and maintains pain as well as other symptoms that are mediated by the central nervous system. It occurs in the absence of proven infection or obvious local pathology accounting for the pain and also occurs in both sexes. It is often associated with negative cognitive behavioural, sexual or emotional consequences as well as with urological, sexual, bowel or gynaecological/prostate dysfunction and has hugely negative impact on quality of life.
In women CPPS occurs unrelated to menstrual cycle, pregnancy or pelvic surgery. Costs of treating CPPS in women estimated at about USD 880 million annually with about 15% of women reporting loss of work days and 45% decreased work efficiency (33)
CPPS prevalence in women ranges from 15-25%. The prevalence of female CPPS varies globally according to the inclusion criteria, but is estimated to affect 6–25 % of women of reproductive age.
CPPS prevalence in men ranges from 2-6% (35). The prevalence of male CPPS varies globally, being estimated at 2-16% in USA and at 2.7- 8.7% in Asia. It usually affects young men (mean age 43 yrs) and presents with perineal and genital pain, which can be unrelenting. While many theories exist, the definitive cause and pathophysiology of male CPPS remain largely unknown (35), which has made management more challenging.
CPP and CPPS are usually challenging to treat. Despite a diagnosis, treatment of the suspected cause often fails to give expected results. This may be due to the multiple presentations and multi-factorial causes and contributing factors. It is therefore agreed that a multidisciplinary and multimodal approach to chronic pelvic pain is most likely to give optimum results. Often a thorough history is key to identifying the cause of the pain and contributing factors.
While there are many causes, one of the musculoskeletal causes of CPP can often be related to the can be deepest layers of PF muscles spasming or becoming dysfunctional. PF muscles often appear to initially trigger the pain of CPP or overwork to compensate for weakness in surrounding muscles. This over activity may then result in spasms, muscle trigger points and hypersensitivity as the muscles try to adapt to maintain function due to weakness in the pelvis-hip-spine complex or even due to disease or conditions in the viscera such as endometriosis or irritable bowel etc. So pain may not resolve until the initial cause or even co-existing causes have been addressed as well as the PF.
Management for CPP includes medications, hormonal therapy, counselling, multi-disciplinary approach to pain management, physiotherapy, psychotherapy, dietary, fluids and behavioural modifications. Successful treatment requires a multimodal and multidisciplinary approach involving pain physicians, obstetricians-gynaecologists, urologists, gastroenterologists, primary care providers, physical therapists, psychiatrists and psychologists

Interstitial cystitis/bladder pain syndrome (IC/BPS) is a chronic, often debilitating, painful condition associated with lower urinary tract symptoms and pelvic pain occuring in the absence of infection or the presence of another disorder (27). There are typically exacerbations, remissions, which vary and fluctuate in in severity. Pain, often worse with bladder filling and relieved by voiding, may centre on the bladder or radiate to the suprapubic area, urethra, or pelvis and may range from tenderness in the lower abdomen or intense pain in the pelvic floor and pain with sex. Symptoms can overlap with other conditions making diagnosis challenging and often time consuming, but other conditions must 1st be excluded making it a diagnosis of exclusion based on patient symptoms.
Despite various theories existing on the cause involving urothelial dysfunction, mast cell activation, neurogenic inflammation, and central nervous system pain perception alterations, none are conclusive and treatments are frequently ineffective. Cystoscopic findings are nonspecific and no objective signs or tests exist to confirm the diagnosis. Hence clinical diagnosis is one of exclusion, based on patient reported symptoms (28).
Most studies show a female-to-male preponderance of 5:1 or greater. Its prevalence ranges from 52 to 5/1000 in females compared to .08–.41/1000 in males, and its incidence is increasing globally (30).
Due to variable presentation it presents challenges that have led to a variety of managements which appear to be best evaluated by a multidisciplinary team. For management to be effective it therefore requires a multimodal approach focused on the individual patient, targeting the symptoms that most impact their quality of life. Suggested strategies are broken down into 5 approaches (31) :-
for mild BPS includes lifestyle modifications i.e. diet, exercise, smoking cessation, stress management, hypnotherapy, acupuncture, cognitive behavioural therapy and physiotherapy e.g. fluids control, timed voiding, bladder training, down training of the pelvic floor, relaxation techniques, myofascial and trigger point release.
1st line – paracetamol and NSAID with gastric protection, 2nd line – Amitriptyline, oral pentosan, Polysulfatesodium or histamine.
or combinations of various bladder instillations.
Intravesical Botox, nerve stimulation – PTNS or SNS or oral Cyclosporine A.
Bladder augmentation cystoplasty or urinary diversion with or without cystectomy.
It is believed that conservative treatment should be the key to BPS management as it is risk free and relatively low cost. Studies show that it can lead to up to 88% improvements in symptoms (31). Given the impact that this condition has, both education and support become hugely important. Involving family or partners during curing appointments can be helpful in providing support. Support groups, cognitive behavioural therapy and alternative therapies can offer valuable help.
In CPP/CPPS patients, the primary goal of Pelvic Health Physiotherapy is to retrain the pelvic floor muscles in order to improve their strength and voluntary relaxation, hence reduce fear of pain and dysfunction that so often inhibits intimacy and sexual activity, increase understanding of condition so as to enable empowerment to control and self-manage the condition, with hope of regaining function and reducing pain. As well as applying the conservative treatment, PTNS and FSM which are both invaluable tools in its management.
The positive effects of the 12-week PTNS treatment for idiopathic OAB symptoms were supported by long-term randomized controlled trials demonstrating persistence of efficacy after 12 and 24 months (29)
The specialist advisers commented that long-term efficacy of PTNS on OAB has not been established and listed key efficacy outcomes as reduced episodes of urgency and urge incontinence, reduced daily pad usage, improvements in quality of life and bladder capacity.
If you suffer from one of the above conditions that can be addressed with Pelvic Health Physiotherapy or would like to consider PTNS as an option for treatment please contact us by email on and request an appointment with Tricia.
Registered and Chartered Physiotherapist
BSc (Hons) HCPC MCSP POGP PG Dip (Women’s Health)
FSM Practitioner
Acupuncturist

To book an appointment, or get in touch with a practitioner, call
Or book an appointment online