In some cases, abdominal adhesions can cause referred pain in other parts of the body, including spinal, abdominal and lower back pain.
Diagnosis of abdominal adhesions typically involves a physical examination, medical history review, and imaging tests, such as an X-ray, ultrasound, CT scan or MRI. In some cases, diagnostic laparoscopy or exploratory surgery may be necessary to confirm the presence of adhesions.
Infections can sometimes lead to the formation of abdominal adhesions, although this is not a common cause. In general, abdominal adhesions are most commonly caused by abdominal surgery or inflammation in the abdominal cavity, such as from conditions like endometriosis or inflammatory bowel disease. However, infections can sometimes lead to inflammation in the abdomen, which can increase the risk of adhesion formation.
Certain types of infections, such as peritonitis (inflammation of the lining of the abdominal cavity), can be particularly concerning for adhesion formation. In peritonitis, inflammation can cause the abdominal organs to stick together and form adhesions, which can lead to chronic abdominal pain.
In general, viruses are not a common cause of abdominal adhesions. However, some viral infections can cause inflammation in the abdominal cavity, which can increase the risk of adhesion formation. For example, viral hepatitis (inflammation of the liver caused by a virus) can cause inflammation in the liver and surrounding abdominal organs, which can increase the risk of adhesion formation.
Other viral infections that can cause inflammation in the abdominal cavity include cytomegalovirus (CMV), Epstein-Barr virus (EBV), and viral gastroenteritis (often caused by norovirus or rotavirus). However, it is important to note that not all cases of viral infections result in inflammation in the abdomen or adhesion formation.
It is also worth noting that in some cases, adhesions may form as a result of multiple factors, including infection, surgery, and inflammation. In these cases, it can be difficult to determine the exact cause of the adhesions.
Scar tissue, including abdominal adhesions, forms as a natural part of the body’s healing process in response to injury or inflammation. When there is damage to tissues in the body, such as during surgery or as a result of infection or inflammation, the body responds by producing fibrous tissue, which eventually forms into a scar. Over time, this fibrous tissue can become thicker and more rigid, which can cause organs to stick together and limit their ability to move freely.
The exact process of scar tissue formation is complex and involves a number of different cellular and molecular mechanisms, including the activation of specialised cells called fibroblasts, the deposition of extracellular matrix proteins, and the formation of new blood vessels.
While scar tissue formation is a natural and necessary part of the body’s healing process, excessive or abnormal scarring can cause a range of problems, including the formation of adhesions. In some cases, adhesions can cause chronic pain and other complications, which may require medical intervention to manage.
The amount of scarring that occurs after an injury or surgery can vary from person to person, and there are several factors that can influence the amount of scar tissue that is produced.
One of the most important factors is the nature and extent of the injury or surgery. More extensive injuries or surgeries that involve larger areas of tissue damage are more likely to produce larger scars. Additionally, injuries or surgeries that involve deeper layers of tissue, such as the muscles or connective tissue, are also more likely to produce more scarring.
Other factors that can influence scarring include genetics, age, and overall health. For example, some people may be genetically predisposed to produce more scar tissue than others. Age can also play a role, as older individuals tend to produce more scar tissue than younger individuals. Additionally, overall health and nutrition can impact scarring, as poor nutrition or underlying health conditions can impair the body’s ability to heal and produce healthy tissue.
Finally, the way in which an injury or surgery is managed can also impact scarring. Proper wound care, including keeping the wound clean and moist, can help reduce scarring. Additionally, some medical treatments, such as the use of steroid injections or topical creams, may also help reduce scarring.
Overall, scarring is a natural part of the body’s healing process, and some degree of scarring is inevitable after an injury or surgery. However, by understanding the factors that can influence scarring, individuals and healthcare professionals can take steps to minimise scarring and promote optimal healing.
Small intestinal bacterial overgrowth (SIBO) is a condition in which there is an abnormal increase in the number of bacteria in the small intestine. While SIBO can lead to a range of digestive symptoms, including inflammation, bloating, gas and diarrhoea, it is not typically associated with the formation of abdominal adhesions.
However, if SIBO it is left untreated over a prolonged period of time or becomes chronic, it can cause adhesions through the ongoing chronic inflammatory processes. It can also lead to other complications, including malabsorption of nutrients and damage to the lining of the small intestine.
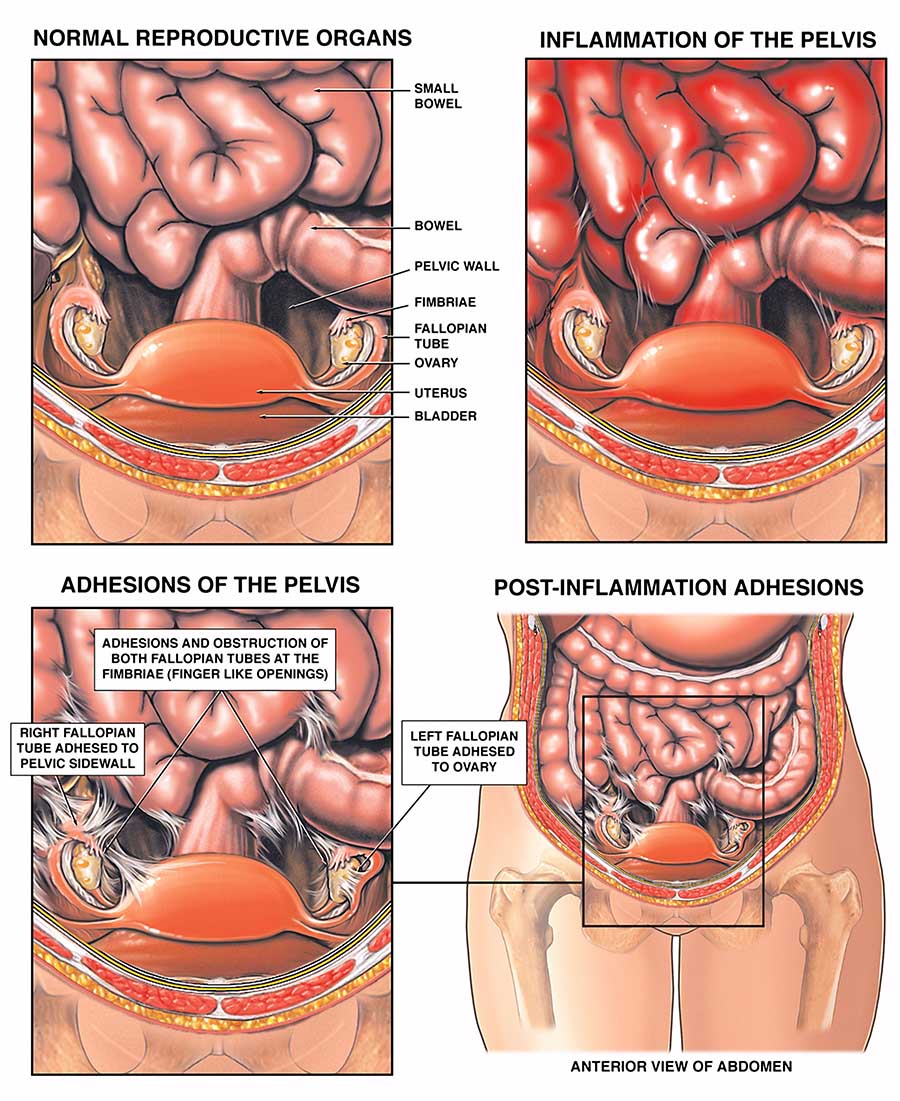
Endometriosis is a chronic condition in which tissue similar to the lining of the uterus (endometrium) grows outside of the uterus, typically on the ovaries, fallopian tubes, and other organs in the pelvis. This tissue can cause a variety of symptoms, including pain, irregular periods, heavy periods, infertility and other symptoms. Additionally, the presence of endometrial tissue outside of the uterus can lead to the development of cysts, called endometriomas, on the ovaries, which can also cause pain and other symptoms.
The exact cause of endometriosis is not fully understood, but it is believed to be related to hormonal and immune system factors. It is also thought to be influenced by genetic and environmental factors.
One of the main ways that endometriosis affects the body is through the formation of adhesions, which are bands of scar tissue that can develop between organs or tissues. As the endometrial tissue grows outside of the uterus, it can invade and damage nearby structures, leading to inflammation and the formation of adhesions. These adhesions can cause pain, discomfort, and infertility by interfering with the normal functioning of the affected organs.
The severity of endometriosis can vary widely from person to person, with some women experiencing mild symptoms while others experience severe pain and infertility. Treatment options for endometriosis include medication, surgery, and lifestyle modifications, depending on the severity of the symptoms and the individual’s goals for treatment.
1. Medications: Over-the-counter pain relievers, such as ibuprofen or paracetamol, can be used to manage pain caused by adhesions.
2. Surgery: In severe cases, surgery may be required to remove the adhesions. However, surgery can also cause new adhesions to form.
3. Physical therapy: Certain exercises and stretches may help reduce pain caused by adhesions and improve mobility.
4. Laparoscopic adhesiolysis: This is a minimally invasive procedure where a surgeon uses a laparoscope to cut and remove adhesions.
5. Adhesion barriers: These are biodegradable materials that can be placed between organs during surgery to prevent new adhesions from forming.
6. Myofascial release is a manual therapy technique that involves applying gentle pressure to release tension and restrictions in the fascia (connective tissue) that surrounds and supports the muscles and organs in the abdomen. Myofascial release may be used as a complementary therapy for abdominal adhesions to help relieve pain and improve mobility.
During a myofascial release session, a therapist will use their hands to apply pressure and stretch the fascia in the abdomen. This can help break up adhesions and scar tissue and improve blood flow and nutrient supply to the affected tissues. Myofascial release may also help improve bowel function and reduce symptoms such as bloating, constipation, and diarrhoea.
While myofascial release may provide some relief for abdominal adhesions, it is important to note that it is not a substitute for medical treatment or surgery when necessary. It is always best to consult with a healthcare professional before trying any new therapies or treatments for abdominal adhesions.
1. Ten Broek RP, Issa Y, van Santbrink EJ, Bouvy ND, Kruitwagen RF, Jeekel J, Bakkum EA, Rovers MM. Burden of adhesions in abdominal and pelvic surgery: systematic review and met-analysis. BMJ. 2013 Apr 18;346:f5588. doi: 10.1136/bmj.f5588. PMID: 23599258.
2. Parker MC, Wilson MS, Menzies D, Sunderland G, Clark DN, Knight AD, Crowe AM. The SCAR-3 study: 5-year adhesion-related readmission risk following lower abdominal surgical procedures. Colorectal Dis. 2005 May;7(3):551-8. doi: 10.1111/j.1463-1318.2005.00823.x. PMID: 15859922.
3. Di Saverio S, Coccolini F, Galati M, Smerieri N, Biffl WL, Ansaloni L, Tugnoli G, Velmahos GC, Sartelli M, Bendinelli C, Fraga GP. Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2017 update of the evidence-based guidelines from the world society of emergency surgery ASBO working group. World J Emerg Surg. 2018 Jan 30;13:24. doi: 10.1186/s13017-018-0179-9. PMID: 29441122; PMCID: PMC5794371.
4. Mazzotta E, De Santis M, Saade GR. Abdominal adhesions: current and novel therapies. J Matern Fetal Neonatal Med. 2011 Dec;24 Suppl 1:35-8. doi: 10.3109/14767058.2011.610182. PMID: 21895517.
5. Brüggmann D, Schmedt N, Klingelhöfer D, Quarcoo D. Surgical procedures and adhesion formation: current understanding of the role of mechanical forces in abdominal adhesion pathogenesis. J Gastrointest Surg. 2015 Apr;19(4):756-66. doi: 10.1007/s11605-015-2753-3. Epub 2015 Feb 24. PMID: 25712206.
6. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 114: Management of Endometriosis. Obstet Gynecol. 2010 Dec;116(6):223-36. doi: 10.1097/AOG.0b013e3181fcdd40. PMID: 21099605.
7. Ballard K, Lane H, Hudelist G, Banerjee S, Wright J. Can specific pain symptoms help in the diagnosis of endometriosis? A cohort study of women with chronic pelvic pain. Fertil Steril. 2010 Dec;94(7):20-7. doi: 10.1016/j.fertnstert.2010.03.025. Epub 2010 May 12. PMID: 20466304.
8. Johnson NP, Hummelshoj L; World Endometriosis Society Montpellier Consortium. Consensus on current management of endometriosis. Hum Reprod. 2013 Feb;28(2):155-70. doi: 10.1093/humrep/des427. Epub 2013 Jan 3. PMID: 23284169.
9. Stratton P, Berkley KJ. Chronic pelvic pain and endometriosis: translational evidence of the relationship and implications. Hum Reprod Update. 2011 Nov-Dec;17(6):327-46. doi: 10.1093/humupd/dmr007. Epub 2011 May 18. PMID: 21596878.
10. Giudice LC. Clinical practice. Endometriosis. N Engl J Med. 2010 Sep 9;362(10): 2389-98. doi: 10.1056/NEJMcp1000274. PMID: 20592295.
11. Pimentel, M. (2018). Evidence-based management of irritable bowel syndrome with diarrhea. The American Journal of Managed Care, 24(14 Suppl), S292-S302.
12. Ghoshal, U. C., & Shukla, R. (2020). Small intestinal bacterial overgrowth and irritable bowel syndrome: A bridge between functional organic dichotomy. Gut and Liver, 14(3), 237-246.
13. Chedid, V., Dhalla, S., Clarke, J. O., Roland, B. C., & Dunbar, K. B. (2017). The epidemiology of small intestinal bacterial overgrowth and its association with irritable bowel syndrome: An overview. The American Journal of Gastroenterology, 112(2), 289-290.
14. Gasbarrini, A., Corazza, G. R., Gasbarrini, G., & Montalto, M. (2018). Small intestinal bacterial overgrowth syndrome: From pathogenesis to clinical practice. Digestive and Liver Disease, 50(7), 640-646.
15. Rezaie, A., Buresi, M., Lembo, A., Lin, H., McCallum, R., Rao, S., … & Pimentel, M. (2017). Hydrogen and methane-based breath testing in gastrointestinal disorders: The North American consensus. The American Journal of Gastroenterology, 112(5), 775-784.